Haftungsausschluss: Dieser Leitfaden dient zu Informationszwecken und stellt keine Diagnose dar. Die hier beschriebenen Behandlungen sind möglicherweise nicht für Long Covid zugelassen und werden von Fall zu Fall geprüft.
Long COVID bedeutet nicht nur, dass „die Genesung länger dauert“.
Leider kann eine COVID-19-Infektion bei vielen Menschen anhaltende Symptome auslösen, die noch drei Monate oder länger nach der Infektion bestehen bleiben. Diese äußern sich in Form von wiederkehrenden, belastenden Symptomen, zu denen Erschöpfung, geistige Trägheit, Schwindel oder Engegefühl in der Brust gehören können.
Im Gegensatz zu anderen Erkrankungen, bei denen man sich mit der Zeit allmählich besser fühlt, verlaufen die Symptome von Long COVID nicht nach dem typischen Genesungsverlauf. Zu verstehen, warum dies geschieht, ist der erste Schritt hin zu einer wirksamen Behandlung und zur Linderung der Symptome.
Warum sich Long COVID nicht wie eine normale Genesung verhält
Normalerweise erholt sich der Körper nach einer Virusinfektion mit der Zeit. Der Post-COVID-19-Zustand stellt einen anhaltenden biologischen Zustand dar. Das Immunsystem, das Gefäßsystem und das Nervensystem bleiben noch lange nach dem Abklingen des Virus dysreguliert, was zu einer beunruhigenden und schwächenden Symptomgruppe führt.
Deshalb scheitern„Ruhe und Zeit“ oft . Anstelle einer stetigen Besserung erleben viele Patienten Rückfälle oder Schübe. Sie können sich eine Woche lang gut fühlen, haben dann aber nach geringfügiger Anstrengung plötzlich wieder Probleme.Dieses Muster lässt sich auch bei anderen chronischen Erkrankungen beobachten, wie zum Beispiel Fatigue chronischen Fatigue oder bei Autoimmunerkrankungen, bei denen Entzündungen und eine schlechte Durchblutung den Körper in einem Teufelskreis gefangen halten.
Zu den häufigsten Nebenwirkungen gehören:
- Anhaltende Fatigue kognitiven Einschränkungen und/oder Beschwerden im Brustbereich.
- Schwierigkeiten bei der Arbeit oder Unfähigkeit, den normalen Tagesablauf aufrechtzuerhalten.
- Eine Reaktion auf körperlichen oder emotionalen Stress, die unverhältnismäßig erscheint.
Es ist wichtig zu beachten, dass Long COVID im Kern biologischer und nicht psychologischer Natur ist.
Das zentrale biologische Problem: Eine Entzündung, die nicht abklingt
Systemische und vaskuläre Entzündungen.
Bei Infektionen kommt es im Rahmen der Immunantwort zur Auslösung einer Entzündung, um das Virus zu bekämpfen; sobald das Virus beseitigt ist, lässt die Entzündung nach und die Heilungsphase beginnt. Bei Long COVID führt eine Fehlregulation des Immunsystems dazu, dass dieser Abschaltmechanismus versagt, wodurch ein Zustand chronischer Entzündung entsteht.
Spuren der Immunaktivierung bleiben insbesondere in Ihrem Gefäßsystem zurück, jenem Netzwerk aus Blutgefäßen, das jede Zelle mit Sauerstoff und Nährstoffen versorgt.
Das Endothel, also die Zellschicht, die diese Gefäße auskleidet, wird gereizt (ein Vorgang, der als Endothelentzündung bezeichnet wird). Die Diagnose ist frustrierend, da die Blutwerte „normal“ erscheinen können, da routinemäßige Blutuntersuchungen weder mikrovaskuläre Belastungen noch eine geringe Zytokinaktivität nachweisen.
Zu den wichtigsten biologischen Veränderungen können gehören:
- Ein Ungleichgewicht der Zytokine (die entzündungsfördernden Signalproteine des Körpers sind erhöht, während die entzündungshemmenden Signalproteine vermindert sind).
- Eine Reizung des Endothels führt dazu, dass die Gefäßwände „klebriger“ werden und sich zudem entzünden.
- Eine beeinträchtigte Mikrozirkulation und Mikrogerinnsel verhindern, dass Sauerstoff und Nährstoffe das Gewebe effektiv erreichen.
Eine Entzündung, die sich selbst aufrechterhält
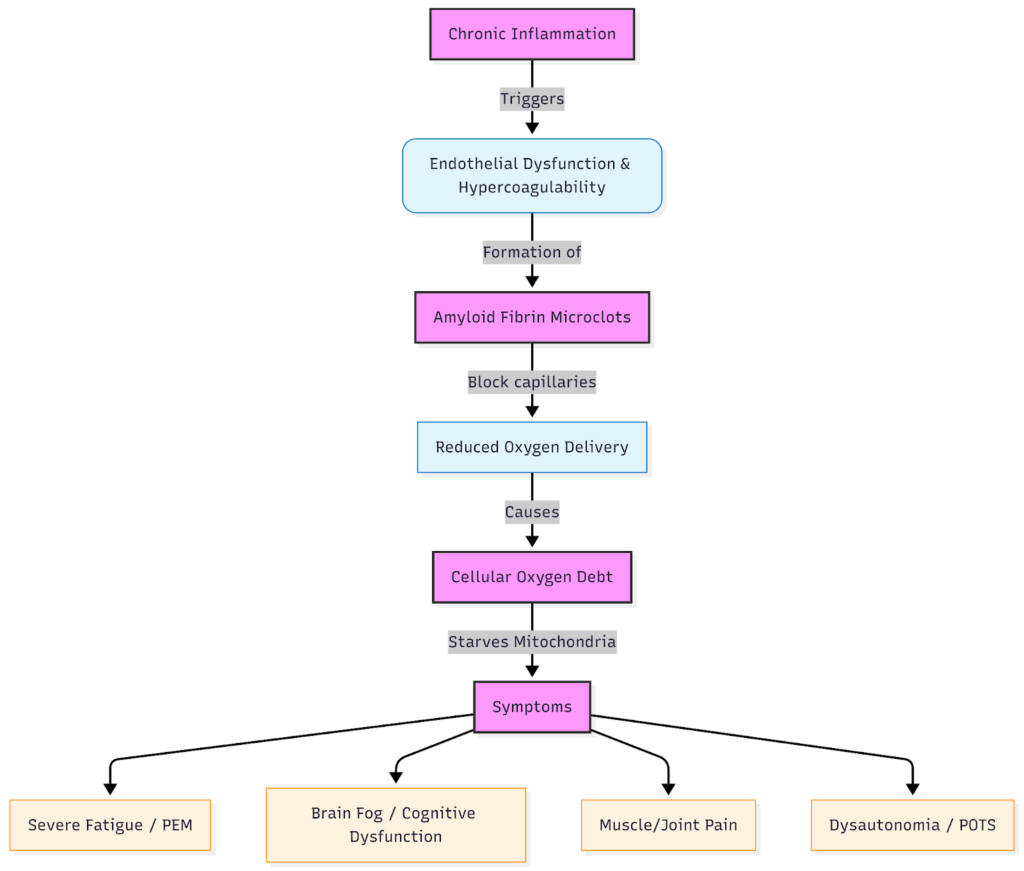
Wenn das Gefäßsystem entzündet ist, kommt es zu einer Beeinträchtigung der Sauerstoffversorgung. Dieser Sauerstoffmangel verschlimmert die Entzündung, führt zu einer Hypoxie und löst einen Teufelskreis aus.
Wenn sich ein Sauerstoffdefizit aufbaut, leiden die Patienten unter stärkerer Fatigue, geistiger Trägheit und Belastungsintoleranz, was oft als post-exertionales Unwohlsein (PEM) bezeichnet wird.
Dieser Mechanismus erklärt, warum es nach hinten losgehen kann, wenn man trotz der Symptome weitermacht oder eine „schrittweise Bewegungstherapie“ versucht. Tatsächlich kann mehr Aktivität die Entzündung verstärken, anstatt die Kraft wieder aufzubauen. Ein schonendes Tempo hingegen hilft dabei, das Energieniveau zu stabilisieren, ohne Rückschläge auszulösen.
Zu den damit verbundenen Symptomen gehören häufig:
- Müdigkeit, die sich durch Ruhe nicht bessert, sondern eher verschlimmert.
- Druckgefühl in der Brust, Atemnot und plötzliche Herzrhythmusbeschleunigung nach geringster Anstrengung.
- Kognitive oder sensorische Überlastung infolge geistiger Anstrengung.
Mikrogerinnsel: Wie der Blutfluss auf kleinster Ebene blockiert wird
Was sind Mikrogerinnsel?
Eine der wichtigsten biologischen Erkenntnisse im Zusammenhang mit Long COVID ist das Vorhandensein von Microclots, also winzigen, widerstandsfähigen Klümpchen im Blutkreislauf. Im Gegensatz zu typischen Blutgerinnseln, die bildgebend sichtbar sind, bilden sich diese Mikrothrombosen auf mikroskopischer Ebene und entziehen sich routinemäßigen Untersuchungen.
Sie stehen im Zusammenhang mit einer Hyperaktivierung der Blutplättchen, was bedeutet, dass die für die Blutgerinnung zuständigen Zellen ungewöhnlich „klebrig“ bleiben. Auch wenn diese Reaktion zunächst schützend wirken mag, führt microclot anhaltende microclot dazu, dass die Sauerstoffversorgung dort beeinträchtigt wird, wo sie am dringendsten benötigt wird.
Wie Mikrogerinnsel den Sauerstoff dort reduzieren, wo er am dringendsten benötigt wird
Kapillaren sind die kleinsten Blutgefäße im Körper, und ein durchschnittlicher Mensch verfügt über eine Gesamtlänge von 60.000 bis 100.000 km. Kapillaren spielen eine sehr wichtige Rolle, denn in ihnen gelangt der Sauerstoff aus dem Blut in das Gewebe. Mikrogerinnsel, die bei Long COVID auftreten, können diese Wege blockieren, was zu einer Gewebehypoxie führt – oder zu dem, was Patienten oft als „Sauerstoffdefizit“ bezeichnen.
Diese Sauerstoffunterversorgung lässt sich oft nicht immer mit einem Pulsoximeter feststellen, da diese Geräte den Sauerstoffgehalt im Blut messen, nicht aber dessen Zufuhr zu den Zellen. Eine venöse Blutgasanalyse kann jedoch manchmal Aufschluss darüber geben, ob Probleme bei der Sauerstoffversorgung vorliegen.
Zu den von Microclots betroffenen Systemen Microclots Ihren Symptomen können gehören:
- Muskeln → schnelle Ermüdung, Schweregefühl, Leistungsabfall nach dem Training.
- Gehirn → Konzentrationsschwäche, Gedächtnislücken, „vernebelte“ Gedanken.
- Vegetatives Nervensystem → Symptome einer Dysautonomie wie Temperaturschwankungen oder Herzrhythmusstörungen.
Sauerstoffmangel: Warum Ihre Zellen auf Reserve laufen
Sauerstoffzufuhr vs. Sauerstoffsättigung
Ihr Pulsoximeter zeigt vielleicht 98 % an, doch Ihre Muskeln und Ihr Gehirn haben möglicherweise dennoch Schwierigkeiten, mit Sauerstoff versorgt zu werden. Diese Diskrepanz zwischen dem Sauerstoffgehalt im Blut und der Sauerstoffversorgung bezeichnet den Zustand der „Sauerstoffschuld“, der bei vielen Long-COVID-Patienten auftritt.
Warum körperliche Anstrengung die Symptome verschlimmert
Körperliche Anstrengung erhöht den Sauerstoffbedarf des Körpers. Wenn Microclots mitochondrialer Stress die Versorgung blockieren, verschlimmern sich die Symptome rasch. Dies ist die Ursache für das post-exertionale Unwohlsein (PEM), das sowohl bei Long COVID als auch bei chronischen Fatigue auftritt, bei denen die Regenerationsmechanismen des Körpers mit dem Energieverbrauch einfach nicht Schritt halten können.
Beteiligung des Nervensystems
Autonome Dysfunktion (Dysautonomie) und POTS
Bei einem Teil der Patienten tritt eine Erkrankung namens Dysautonomie auf, bei der das autonome Nervensystem, das Herzfrequenz, Blutdruck und Verdauung steuert, nicht mehr richtig funktioniert.
Viele leiden unter orthostatischer Intoleranz (Ohnmachtsgefühl beim Aufstehen) und POTS (posturales orthostatisches Tachykardiesyndrom) oder unter Schwankungen der Körpertemperatur.
Zu den Symptomen können gehören:
- Herzklopfen oder schneller Herzschlag beim Aufrichten.
- Schwindel oder Fatigue Stehen in Warteschlangen.
- Hitzeunverträglichkeit oder schwankende Raumbedingungen.
Kleinfaser-Neuropathie und MCAS
Unter einer Neuropathie der kleinen Nerven versteht man eine Schädigung oder Entzündung der winzigen Nerven, die für die Wahrnehmung von Berührungen und Temperaturen zuständig sind. Sie kann sich in Form von Brennen, Kribbeln oder einer Reizüberflutung äußern. Darüber hinaus kann das Mastzellaktivierungssyndrom (MCAS) aufgrund einer übermäßigen Aktivität der Immunzellen Hitzewallungen, Hautausschläge, Histaminintoleranz und geistige Trägheit auslösen.
Warum die übliche Behandlung von Long COVID oft zu kurz greift
Die konventionelle Behandlung konzentriert sich hauptsächlich auf die Symptomlinderung durch Herzfrequenzkontrolle, Medikamente und unterstützende Therapien. Diese Methoden tragen zwar zur Stabilisierung bei, gehen jedoch selten auf die biologischen Ursachen wie Entzündungen oder Microclots ein.
Wichtig ist, dass eine stufenweise Bewegungstherapie für Menschen mit PEM Risiken bergen kann, da sie die Leistungsfähigkeit eher verschlechtern als wiederherstellen kann.
Warum die Blutfiltration bei Long COVID untersucht wird
Therapeutische H.E.L.P.-Apherese ist eine Form der Blutfiltration, die in spezialisierten Zentren angewendet wird, um schädliche Substanzen wie Entzündungsproteine, Gerinnungsstoffe oder abnormale Lipide zu entfernen.
Im Zusammenhang mit Long COVID wird HELP (Heparin-induzierte extrakorporale LDL-Präzipitation) eingesetzt, um:
- microclot verringern.
- Entfernen Sie Entzündungsmediatoren.
- Die Mikrozirkulation verbessern.
Erfahren Sie mehr über die umfassende Long-COVID-Therapie.
Was ist das Ziel HELP ?
Bei diesem Verfahren wird das Plasma selektiv gefiltert, um Folgendes zu entfernen:
- Mikrogerinnsel.
- Entzündungsproteine.
- Überschüssige Lipoproteine, die eine Reizung des Endothels verstärken können.
Dieser Ansatz ist nach wie vor ein Spezialverfahren und wird sorgfältig individuell angepasst; er stellt keine Erstbehandlung dar. Jeder Patient muss einer gründlichen Untersuchung unterzogen werden, um die Sicherheit und Eignung sicherzustellen.
Apherese-Verfahren
Wer kommt als Kandidat in Frage (und wer nicht)?
Eine therapeutische Apherese kann bei Patienten mit folgenden Erkrankungen in Betracht gezogen werden:
- Anhaltende, mehrere Organsysteme betreffende Long-COVID-Symptome, die auf eine mikrovaskuläre Entzündung hindeuten.
- Labor- oder klinische Anzeichen einer endothelialen Dysfunktion.
- Eine verminderte Lebensqualität trotz Standardtherapien.
Es ist nicht geeignet für Personen mit:
- Aktive Blutungen oder Gerinnungsstörungen.
- Instabile Herz-Kreislauf-Erkrankungen.
- Bestimmte Medikamentenkombinationen, die das Risiko erhöhen.
Vor der Entscheidung über die Eignung ist eine fachärztliche Beratung unerlässlich.
Was dies für Patienten mit Long-COVID bedeutet
Fragen, die Sie mit Ihrem Arzt besprechen sollten
- Könnten anhaltende Entzündungen oder Microclots zu meinen Symptomen beitragen?
- Welche Untersuchungen könnten bei der Beurteilung einer vaskulären oder autonomen Dysfunktion hilfreich sein?
- Wäre eine Überweisung an eine auf Long-COVID spezialisierte Klinik oder eine Apherese-Sprechstunde angebracht?
Wie wir die Ursache und nicht nur die Symptome behandeln
Unser Ansatz der Kombinationstherapie kombiniert:
- H.E.L.P. zur selektiven Entfernung von Spike-Protein, Microclots und Entzündungsmarkern
- Inusphérese oder Immunadsorption zur Entfernung von Krankheitserregern, Umweltgiften und Autoantikörpern
- Nutrazeutische Mittel & Klinische Ernährungstherapie zur Unterstützung der Reparatur der Mitochondrien und des Immunsystems
- Hyperthermie (wenn angezeigt) zur Stimulierung der Immunmodulation
Erfahrungsberichte von Patienten
„Ich war bei mehreren Ärzten, bevor ich ins Apheresezentrum kam. Sie sagten mir, es sei nur Stress. Nachdem mein microclot positiv ausfiel, hatte ich endlich einen Beweis – und einen Plan.“
— Robyn, Großbritannien
„Die Apherese hat alles verändert. Nach sechs Sitzungen klärte sich mein Gehirnnebel auf und ich konnte endlich arbeiten, ohne das Gefühl zu haben, zusammenzubrechen.“
— Mia, Norwegen
Der nächste Schritt
Wenn Sie sich auch Monate nach einer COVID-19-Erkrankung noch unwohl fühlen, sind Sie nicht allein, und Sie bilden sich das nicht nur ein. Das Verständnis der biologischen Ursachen dieser Symptome eröffnet neue Wege zur Genesung.
Wenn Sie eine individuelle Beurteilung wünschen oder mehr über die therapeutische Apherese bei Post-COVID-19-Symptomen erfahren möchten, vereinbaren Sie noch heute einen Beratungstermin im Apherese-Zentrum.
FAQ: Biologie und Behandlung von Long COVID
Ist Long COVID entzündlicher oder autoimmuner Natur?
Aktuelle, von Fachkollegen begutachtete wissenschaftliche Erkenntnisse zeigen, dass Long COVID eine Kombination aus chronischen Entzündungen und Immunproblemen darstellt und bei manchen Patienten Merkmale von Autoimmunreaktionen aufweist, anstatt sich eindeutig einer einzigen Kategorie von „Autoimmunerkrankungen“ zuzuordnen.
Forscher haben eine anhaltende endotheliale Dysfunktion sowie ein Ungleichgewicht bei Zytokinen und fibrinamyloiden Microclots festgestellt, was insgesamt auf einen lang anhaltenden Entzündungszustand hindeutet. Bei einigen Patientengruppen treten zudem Autoantikörper und eine Neuropathie der kleinen Nervenfasern auf, was in einer bestimmten Anzahl von Fällen auf einen autoimmunen Faktor hindeutet.
Warum sind meine Untersuchungsergebnisse unauffällig, obwohl ich mich immer noch unwohl fühle?
Standardmäßige pathologische Untersuchungen und bildgebende Verfahren konzentrieren sich häufig auf Probleme der großen Gefäße und akute Entzündungen. Das bedeutet, dass mikrovaskuläre Veränderungen, autonome Dysfunktionen oder Neuropathien der kleinen Nervenfasern bei routinemäßigen pathologischen Untersuchungen leicht übersehen werden können. Long COVID geht häufig mit mikroskopisch kleinen Microclots einher, Microclots mit endothelialer Dysfunktion und autonomen Unregelmäßigkeiten wie POTS, die bei Standarduntersuchungen nicht festgestellt werden. Aus diesem Grund wird vielen Patienten mitgeteilt, ihre Ergebnisse seien „normal“, obwohl sie weiterhin unter behindernden Symptomen leiden.
Können Impfstoffe das Risiko für Long COVID verringern?
Mehrere groß angelegte Beobachtungsstudien haben gezeigt, dass eine Impfung vor einer Infektion das Risiko senkt, an einer Post-COVID-19-Erkrankung zu erkranken, auch wenn sie dieses Risiko nicht vollständig ausschließt. Die WHO und andere Gesundheitsorganisationen betonen, dass die Impfung nach wie vor eines der wichtigsten Mittel ist, um das Risiko und den Schweregrad von Long COVID zu verringern.
Autoren-/Medizinischer Gutachtervermerk
Verfasst von Andrew Smith. Überprüft von Dr. Inbar Tofan, Ärztlicher Direktor am Apheresezentrum. Dr. Inbar verfügt über mehr als 10 Jahre klinische Erfahrung in der Inneren Medizin und der therapeutischen Apherese und ist auf chronisch-entzündliche und Autoimmunerkrankungen spezialisiert.